
Most adults with ADHD need both coaching and therapy: coaching builds systems, therapy addresses the shame and perfectionism that keep systems from sticking.



Key Takeaways
For most adults with ADHD, the right answer is not coaching or therapy but both, weighted differently depending on the week.
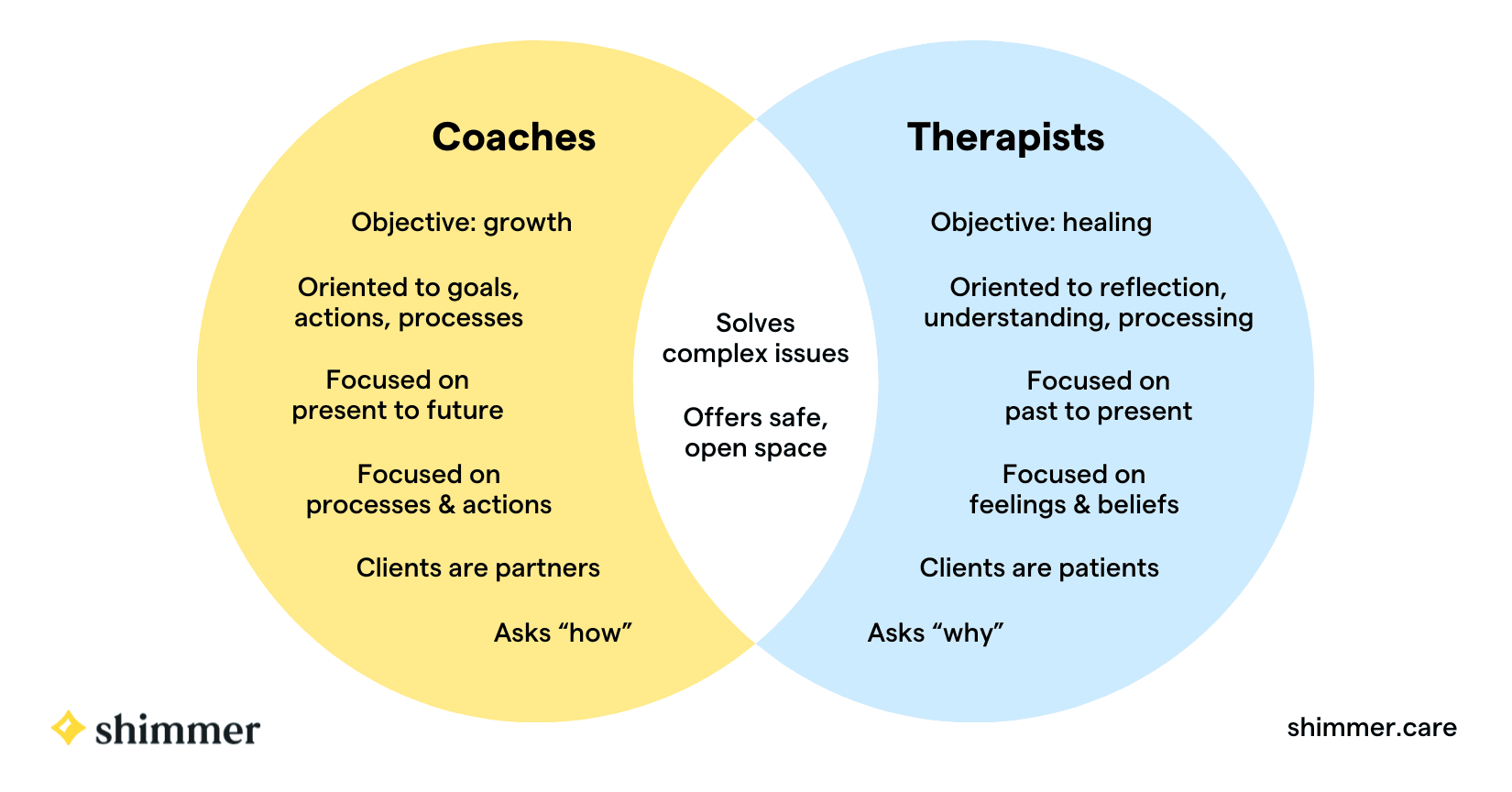
Coaching builds practical scaffolding: planners, routines, systems, accountability. Therapy works on the emotional layer underneath: shame, perfectionism, rejection sensitivity, and the inner critic.
Coaching alone often hits a ceiling fast because systems get abandoned for emotional reasons the coach cannot address; therapy alone often leaves the person insightful and still missing deadlines.
Coaching alone is enough for a specific population: those who have done substantial emotional work, who have mild presentations, or who are in clear time-limited projects.
Therapy alone is the right starting point when the presenting concern is primarily emotional, when the person is in acute distress, or when diagnostic clarity has not yet been established.
Medication, prescribed by psychiatrists, is a complementary intervention that makes both coaching and therapy more effective by giving the brain enough attention regulation to use the tools each is teaching.
For most adults with ADHD, the right answer is not coaching or therapy but both, weighted differently depending on the week. Coaching builds the practical scaffolding that ADHD makes hard: planners, routines, systems, accountability. Therapy works on the emotional layer underneath: the shame, perfectionism, rejection sensitivity, and inner critic that have usually grown up alongside the executive function differences. Coaching alone often hits a ceiling fast because the systems get abandoned for emotional reasons the coach cannot address. Therapy alone often leaves the person insightful and still missing deadlines. The combined approach is what the evidence base recommends, and it is what most adults with ADHD eventually figure out they need.
I'm Dr Rick Smith, PsyD | EdD, a clinical psychologist in Central Hong Kong working with international school families, executives, and high-performing adults on ADHD, executive functioning, anxiety, and performance psychology. A substantial part of my caseload is people with ADHD who have tried one approach and found that on its own it was not enough. The question of where to start is one of the most consequential decisions in adult ADHD care, and it is one of the most poorly explained in the public conversation about it.
What is ADHD coaching, and what does it actually do?
ADHD coaching focuses on the practical, observable, behavioural side of ADHD: the day-to-day work of starting tasks, finishing tasks, planning, remembering, transitioning between activities, managing time, and building routines that hold. A good ADHD coach helps you design external scaffolding to compensate for the executive function differences ADHD creates: visual planners, implementation intentions, body doubling, environmental design, friction in the right places and ease in the others. Coaching is usually goal-oriented and forward-looking; each session reviews what worked, what did not, and what to try next. The relationship is collaborative and often warm, but the focus is on doing rather than on understanding. For many adults, this work overlaps closely with general procrastination and time management work. One important caveat: many ADHD coaches do not require any clinical training, which means quality varies widely. Some are excellent. Some are essentially organisational tips with a billing rate. The lack of regulation in coaching means the responsibility for assessing quality sits with the client, and the variability is much wider than in clinical psychology. When ADHD coaching is done well, it is genuinely transformative for people whose presentation is primarily executive in nature. When it is done poorly, or applied to a presentation that needs clinical work, it can produce months of effort and no durable change.
What is ADHD therapy, and how does it differ from coaching?
ADHD therapy works on the emotional and psychological layer underneath the behavioural difficulties. Almost everyone with ADHD carries some version of the same package by adulthood: a history of being told they are lazy, careless, or not trying hard enough, a self-narrative that confuses effort with worth, rejection sensitivity that makes feedback feel catastrophic, perfectionism that paradoxically makes starting feel impossible, and a harsh inner critic that has been on duty since childhood. These patterns are not solved by a better planner. They require clinical work, usually drawing on cognitive behavioural therapy, acceptance and commitment therapy, and sometimes schema-informed approaches, alongside the standard treatment of the depression and anxiety that often sit beside ADHD. Clinical training matters here because some of the patterns that present as ADHD are actually anxiety, trauma, or learning differences in disguise, and the wrong target wastes years. A clinical psychologist working with ADHD does the assessment work first, gets the diagnosis right, identifies what is ADHD and what is something else, and then treats the actual condition rather than the assumed one. This is the layer of work that ADHD coaches generally cannot provide, not because they are unwilling but because diagnostic skill requires clinical training. For most adults who arrive at clinical work having tried coaching first, the missing piece is usually this clinical layer, and adding it is what makes the coaching gains sustainable.
Why do most people with ADHD benefit from both at once?
Most people with ADHD benefit from both because the executive function difficulties and the emotional layer reinforce each other in both directions, and addressing only one leaves the other intact to undo the gains. Better systems reduce shame; less shame makes systems usable. Coaching without the emotional layer often hits a ceiling fast because the underlying perfectionism and rejection sensitivity make using the system feel exposing. Opening the planner means facing the to-do list, which means feeling the weight of everything not yet done, which triggers the inner critic, which makes the situation intolerable, which makes closing the planner feel like relief. The system was never the problem; the emotional cost of using it was. The opposite pattern also happens. Adults who work for a year or two with a kind, skilled therapist often feel more compassionate toward themselves and clearer about their patterns, and are still missing deadlines and losing keys. Insight does not transfer to executive function. ADHD is not solved by understanding ADHD; the brain still does the thing it does. The therapists who are most effective for ADHD blend clinical work with concrete behavioural interventions: implementation intentions, externalised planning, environmental design, accountability structures. Without that, therapy can be deeply useful for the person's relationship with themselves and largely useless for the day-to-day chaos. The evidence base for adult ADHD treatment recommends an integrated approach combining executive function skills work with the emotional and cognitive layer, because both layers are usually present and both need to be addressed to produce durable change. For ADHD and executive function coaching delivered alongside clinical work, this integration is the central principle of how I structure sessions.
When is coaching alone enough, and when is therapy alone the right starting point?
Coaching alone is enough for a specific population, and the conditions matter. The first is that the person has already done substantial emotional work; the shame layer is small, the self-narrative is reasonably healthy, and they mostly need someone to help them design and maintain systems. The second is mild presentation; ADHD exists on a spectrum, and some people have meaningful executive function differences without the emotional comorbidity that more severe presentations bring. The third is a clear, time-limited goal: finishing a thesis, launching a business, getting through a high-stakes period. The fourth is an already-established therapy relationship that handles the emotional work, with coaching as a separate complementary intervention. When these conditions are present, coaching alone can be a strong fit. Therapy alone is less common but happens in specific situations. The first is when the presenting concern is primarily emotional, such as persistent low mood, anxiety, or self-criticism that may relate to ADHD but is not currently about task completion. The second is acute distress, when the inner critic is loud, depression is present, or rejection sensitivity is causing daily collapse; building a planner first will not work because the emotional ground has to settle before the practical scaffolding has anywhere to land. The third is diagnostic uncertainty. If it is not yet clear whether the presentation is ADHD, anxiety, autism, depression, or some combination, the assessment and formulation work that clinical psychologists are trained in usually has to come first. Coaches generally cannot do this. For most adults, neither pure scenario applies, and the integrated approach is the right one.
How do you actually decide where to start with ADHD support?
Five questions usually clarify the decision. The first is whether you have a longstanding pattern of starting strong with new systems and abandoning them. If yes, you probably need therapy alongside coaching, because the abandonment pattern is rarely about the systems. The second is whether there is a significant emotional layer including anxiety, low mood, harsh self-criticism, rejection sensitivity, or perfectionism. If yes, start with therapy or a combined approach. The third is whether you are in a high-stakes time-limited project where you need structure now. If yes, coaching can carry you through the project with therapy considered afterward. The fourth is whether diagnostic clarity is unclear. If yes, start with a clinical psychologist or psychiatrist, because coaches generally cannot disentangle ADHD from anxiety, autism, or trauma. The fifth applies to parents of adolescents. In most cases the combined approach is the right one, because teenagers with ADHD almost always have an emotional layer that needs attention, even when the parents are mainly concerned about homework. For families navigating both layers alongside anxiety patterns that have grown up around the ADHD, the integrated approach is almost always more effective than treating either condition in isolation. If you are unsure where to start, a clinical psychologist with ADHD expertise can usually tell you within two sessions whether your situation calls for pure coaching, pure therapy, or a combined approach. The right answer depends on your specific presentation, not on which camp's marketing reached you first.
The honest summary is that the public conversation about ADHD has split into two camps that mostly mislead the people they are supposed to help. Coaching alone is enough for a small population and insufficient for most. Therapy alone is enough for an even smaller population. Most adults with ADHD need both, ideally in the same room with the same practitioner, weighted toward whichever layer is more pressing in any given week. If you have tried one and found it was not enough, that is the most useful piece of diagnostic information you have, and the answer is usually to add the layer that was missing rather than to keep doubling down on the layer that did not work alone.
Frequently Asked Questions
What is the difference between ADHD coaching and ADHD therapy?
ADHD coaching focuses on the practical, behavioural side: starting and finishing tasks, planning, building routines, designing external scaffolding to compensate for executive function differences. ADHD therapy works on the emotional and psychological layer underneath: shame, perfectionism, rejection sensitivity, inner critic patterns, and the self-narrative that has usually grown up alongside the executive function difficulties. Coaching is goal-oriented and forward-looking; therapy is clinical and addresses the emotional ground the systems are trying to sit on top of.
Why do most adults with ADHD need both coaching and therapy?
Because the executive function difficulties and the emotional layer reinforce each other in both directions, and addressing only one leaves the other intact to undo the gains. Better systems reduce shame; less shame makes systems usable. Coaching without therapy often fails because perfectionism and rejection sensitivity make using the system feel exposing. Therapy without coaching often leaves people insightful and still missing deadlines, because insight does not transfer to executive function on its own.
When is coaching alone enough for adult ADHD?
When the person has already done substantial emotional work, when the presentation is mild without significant emotional comorbidity, when the goal is a clear time-limited project rather than a longstanding pattern, or when there is an established therapy relationship already handling the emotional layer alongside the coaching. When these conditions are present, coaching alone can be a strong fit. Outside these conditions, coaching alone tends to hit a ceiling fast.
When is therapy alone the right starting point?
When the presenting concern is primarily emotional, such as persistent low mood, anxiety, or self-criticism that may relate to ADHD but is not currently about task completion. When the person is in acute distress and the emotional ground has to settle before practical scaffolding has anywhere to land. When diagnostic clarity is unclear and the assessment work that clinical psychologists do has to come first. For most adults with ADHD, neither pure scenario applies, and the integrated approach is the right one.
Can an ADHD coach diagnose ADHD?
No, diagnosis requires specific training in standardised assessment instruments and clinical interviewing. ADHD coaches are not generally trained in this and the ethical ones do not claim to be. If you suspect ADHD but do not have a diagnosis, start with a clinical psychologist or psychiatrist. The lack of regulation in the coaching field means quality varies widely; the diagnostic question in particular should sit with someone who has clinical training.
What about medication for ADHD?
Medication is a separate question and usually a complementary one. Stimulant medication, when it suits the person, makes both coaching and therapy more effective by giving the brain enough attention regulation to actually use the tools each is teaching. Medication is prescribed by psychiatrists; psychologists do not prescribe but routinely coordinate with prescribing colleagues. For moderate to severe presentations, combined treatment (medication plus integrated coaching and therapy) typically outperforms any single intervention alone.
Author bio
I'm Dr. Rick Smith, a clinical psychologist in Hong Kong working with high-performing teens and adults on ADHD, anxiety, OCD, addiction, and executive functioning. My work draws on Acceptance and Commitment Therapy, Cognitive Behavioural Therapy, and Exposure and Response Prevention, applied to international school families and the expatriate community.
Before psychology, I spent nearly two decades in classrooms supporting students with learning differences. I'm the author of STOP Reading (4.8 stars on Amazon) and deliver workshops for schools and organisations across the region. More at rick-smith.com.